
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article a Pelvic Rehabilitation Medicine Clinical Research Foundation, West Palm Beach, FL, USA, b The Feinstein Institute for Medical Research, Manhasset, NY, USA, c NYU Langone Medical Center, Rusk Rehabilitation, New York, NY, USA *Corresponding author. Address: Pelvic Rehabilitation Medicine Clinical Research Foundation, 2090 Palm Beach Lakes Blvd, Suite 700, West Palm Beach, FL 33409, Tel.: (561) 805-3875; fax: (561) 318-0134. E-mail address: [email protected] (S. Patil). Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain. This is an open access article distributed under the Creative Commons Attribution-NoDerivatives License 4.0 (CC BY-ND) which allows for redistribution, commercial and non-commercial, as long as it is passed along unchanged and in whole, with credit to the author.
1. Introduction
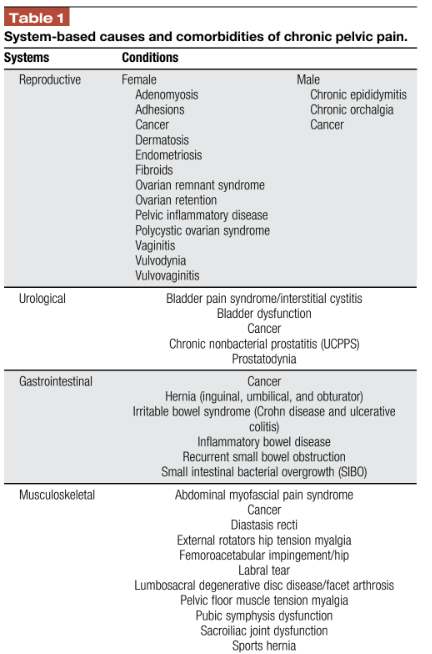
Chronic pelvic pain (CPP) is described by the American College of Obstetricians and Gynecologists as noncyclic “pain symptoms perceived to originate from pelvic organs or structures typically lasting more than 6 months” or cyclical pain that has “significant cognitive, behavioral, sexual, and emotional consequences.”6 Chronic pelvic pain is a multifactorial problem potentially caused by the complex interplay of gynecological, gastrointestinal, urological, musculoskeletal, neurological, and psychosocial conditions among others.4,99 The differential diagnosis is extensive (Table 1). Chronic pelvic pain is one of the most common pain conditions affecting women and can severely affect the quality of life, including physical functioning, psychological well-being, and interpersonal relationships.39 The estimated prevalence for women of reproductive ages is between 14% and 24%, and about 14% percent of women experience CPP during their life.10,87 Urological chronic pelvic pain syndrome affects 2% to 16% of men worldwide.31
Chronic pelvic pain represents a significant individual and societal burden. Although researchers discuss the substantial psychosocial and economic impact on up to 30% of women worldwide, a precise prevalence among both genders is hard to determine because of the lack of multidisciplinary studies and limited understanding or consensus regarding CPP among researchers and health providers.3 Chronic pelvic pain patients often obtain insufficient relief of their symptoms, consult many doctors without obtaining a precise
diagnosis or appropriate management, and can have the impression of being abandoned by the medical profession.96Understanding the complex, multifactorial clinical image of CPP can help physicians determine the pain’s etiology to advise the patient regarding their options for management and which specialists to include in the multidisciplinary care team required for this multifaceted condition. It is also important to keep in mind the biopsychosocial approach and shared decision model with this patient population.15,44 The purpose of this review is to provide a comprehensive overview of the etiology, diagnosis, and treatment options currently available for the management of CPP.
2. Methods
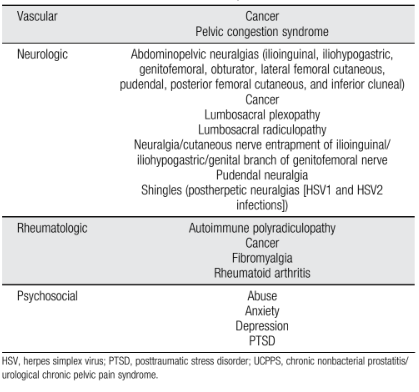
In this narrative review, a literature search was performed using PubMed to identify relevant studies based on the authors’ clinical report on the anatomy and diagnosis of CPPS and (2) report on pharmacological, integrative, or nonsurgical interventional procedures. We excluded articles that (1) were not peer-reviewed articles, (2) related exclusively to acute pelvic pain, (3) studied pelvic pain relating to an active pregnancy, (4) focused on malignancy, (5) used hormonal treatments, and (6) focused on surgical pain management. A total of 502 references were obtained from the search between 1992 and 2020. After eliminating duplicate records (n 5 152), 350 references remained. These records were all screened, and 253 irrelevant studies were excluded. The remaining 97 full-text articles were assessed for eligibility. Of these, 22 articles did not meet the inclusion criteria. Additional studies were located by searching the reference list of the 75 studies. Forty-one new studies met the inclusion criteria, bringing the total to 116 studies included in the review (Fig. 1).
3. Etiology The complexity inherent in CPP suggests that some potential combination of underlying peripheral and central nervous system pathophysiology may be the best approach to diagnosis resulting in a better understanding of the condition itself.110 Central sensitization involves increased membrane excitability and synaptic efficacy in response to normally benign (allodynia) or nociceptive (hyperalgesia) stimuli. This results from neural plasticity within the central nervous system after exposure of the sensory pathway to prolonged inflammation or another neural insult.111 The phenomenon of central sensitization includes alterations of sensory processing within the brain, decreased inhibition of nociceptive pathways, upregulated facilitatory pain pathways, and long-term potentiation of pain-mediating synapses in the brain.75
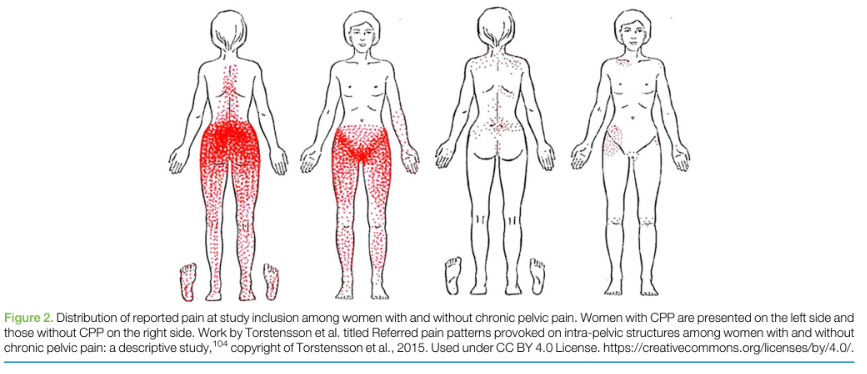
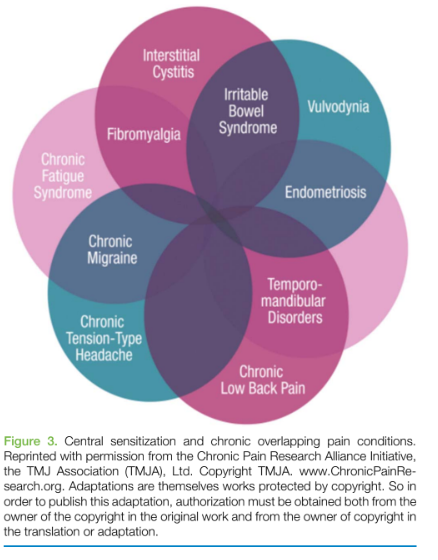
Central sensitization is essentially the uncoupling of the sensation of pain from the presence or intensity of a noxious stimulus because of changes in the properties of neurons within the central nervous system. In addition, central sensitization has been said to include primary and secondary hyperalgesia. In this classification, primary hyperalgesia refers to a decreased nociceptive threshold for firing along with a prolonged, more intense response to noxious stimuli. Secondary hyperalgesia, in contrast, describes the expansion of the painful zone to the surrounding undamaged tissue.111 Torstensson et al.104 demonstrated this by pain mapping in women with and without CPP as depicted in Figure 2. Peripheral sensitization is an increased sensitivity to afferent nerve stimuli.72 Injury or trauma leads to the development of a sensitizing “inflammatory soup,” in which the nerve endings are surrounded by proinflammatory cytokines such as substance P and bradykinin. The presence of this “inflammatory soup” for a long period leads to neuroplasticity and mRNA changes in the peripheral nociceptors. This ultimately causes both a reduction in the threshold for peripheral nociceptors to fire and a heightened response when they do.12 A recent study demonstrated the effects of altered peripheral nerve function as an important pathogenic factor of irritable bowel syndrome (IBS). In patients with IBS, mucosal biopsy supernatants consistently activated enteric and sensory neurons by the synergistic effects of proteases and other neuroactive components, such as histamine and serotonin.23 Given the underlying central sensitization and peripheral sensitization, there is a high presence of chronic overlapping pain syndromes in this patient population of CPP. Chronic overlapping pain syndromes refers to the recognition that
highly widespread chronic pain conditions, such as IBS, endometriosis, temporomandibular disorder, and vulvodynia to name a few, appear to coexist68 (Fig. 3). The phenomenon of viscero-somatic convergence is common in the chronic pain patient population where the visceral pain affects somatic tissues in the referred area because of the
convergence of visceral and somatic afferent fibers on the same spinal sensory neurons, also known as “convergence facilitation.”45 Conversely, pelvic organ “crosstalk,” or visceral–visceral cross sensitization, corresponds to the secondary symptomatic impact on adjacent organs by a “crosssensitization” phenomenon. Pelvic organ crosssensitization is considered a contributing factor in CPP. Crosssensitization refers to the transmission of nociceptive signals from an area that has received, or is receiving, an insult to an adjacent, uninvolved, structure, causing dysfunction in the healthy organ or structure.83 For example, patients with IBS have significantly higher rates of bladder dysfunction such as nocturia, frequency and urgency of micturition, and incomplete bladder emptying.103 This phenomenon occurs by shared sensory pathways within the dorsal root ganglia, spinal cord, or brain. Each of these 3 levels of the nervous system, alone or in combination, is believed to coordinate crosssensitization in the pelvis. Transient receptor potential vanilloid 1 receptors have been implicated in the development of neurogenic inflammation and crosssensitization
in the pelvis and pelvic organs.69
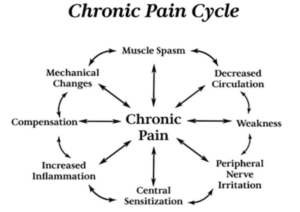
Myofascial pain has a prevalence range from as low as 14% to 23% in women with CPP to as high as 78% among women with bladder pain syndrome or interstitial cystitis.79 A hallmark of its presence are myofascial trigger points (MTrPs) which are focal areas of palpable taut bands found in skeletal muscle that are hypersensitive to palpation and can reproduce the patient’s symptoms with both local and referred pain responses. They can be associated with autonomic symptoms, such as sweating, lacrimation, flushing, vasomotor reactions, and temperature changes.21 Myofascial trigger points are commonly found in many chronic pain conditions including urological chronic pelvic pain syndrome.8 With pelvic pain, patients can experience a deep, aching sensation in a discrete location or with a regional distribution.22 In hypertonic pelvic floor dysfunction, the muscles are short, spastic, and weak with palpable MTrPs. Chronically contracted, weak muscles can lead to a local restriction in blood flow and a change in the environmental pH, which will in turn trigger the inflammatory cascade and perpetuate or cause neurogenic inflammation85 (Fig. 4). In addition to MTrPs, authors have considered the deep fascia and epimysium as potential pain generators. This is due to the dense neuronal innervation with nonpeptidergic nerve fiber endings and the encapsulated mechanoreceptors which are restricted by the surrounding collagen fibers and fibrous stroma in dysfunctional deep muscle fascia.35,98
4. Diagnosis
As there is a variety of gender-specific and organ-specific causes that can lead to CPP, a complete history and physical examination are vital for uncovering potential underlying causes to be addressed. From the musculoskeletal perspective, it is important when listening to a patient’s history to constantly ask “Why is this patient suffering from CPP?” (Table 1). Assessing if a patient’s history suggests an underlying gastrointestinal, urological, gynecological, vascular, psychologic, rheumatologic, musculoskeletal, or neurological cause and bringing in the appropriate specialist consultants can aid in diagnosis.6 This can be challenging as often there is significant overlap between organ systems.
Conducting physical examinations is a key to evaluate the patient, but they can be a potential cause of distress due to prior trauma and/or the psychological impact of these pain conditions. It is vital to carry a trauma-informed model of care while performing the examinations to allow improved communication and avoid stigmatization.25 We achieve this by asking patients for their informed permission and fully explaining the procedure of the examination before conducting it. For minors, an adult chaperone is always present.
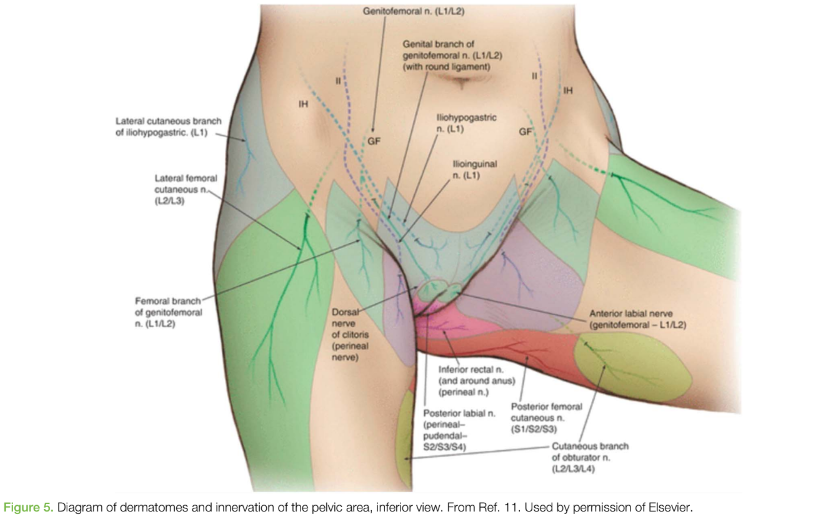
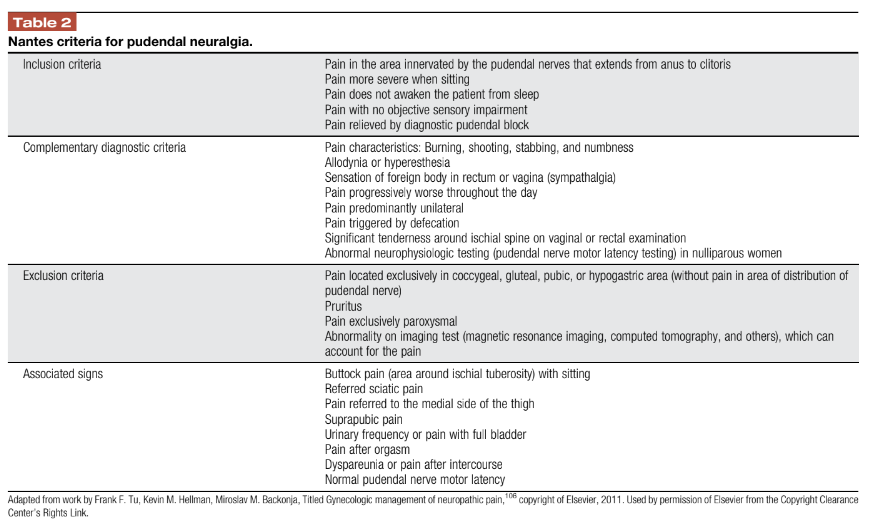
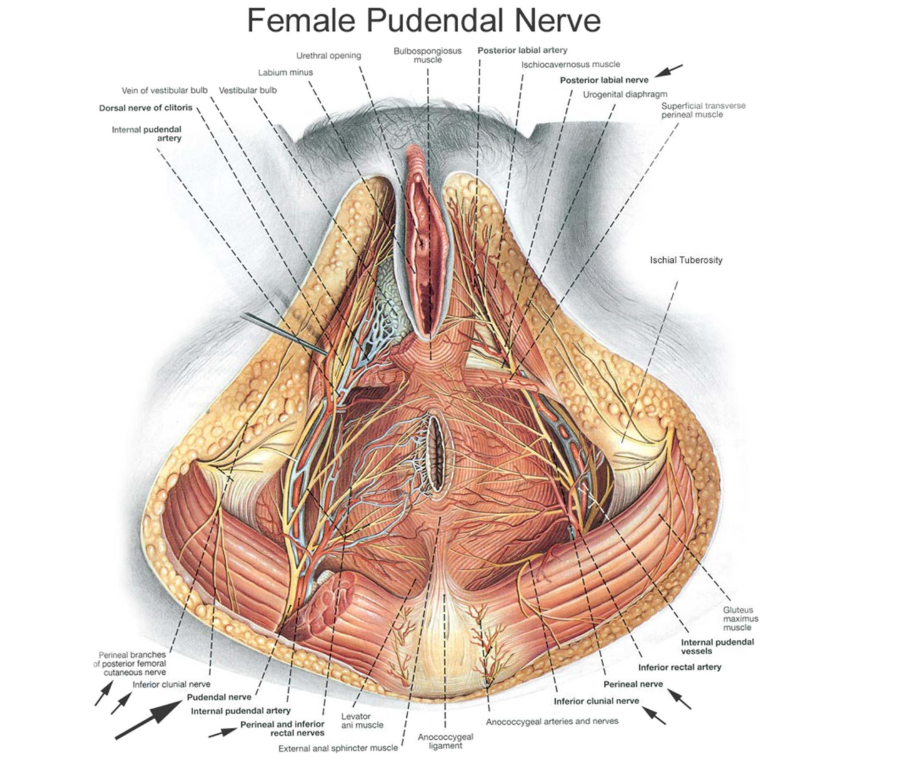
Owing to the complex anatomy contributing to CPP, such as the lumbar and sacral nerve roots supplying the pelvic floor (Fig. 5), a complete physical examination for CPP includes a full lumbosacral examination to evaluate for lumbar radiculopathy, lumbar discogenic pain, lumbar facet pain, sacroiliac joint pathology, or coccydynia. A bilateral hip examination is performed to evaluate for underlying intra-articular or extra- articular hip and pelvic girdle pain generators such as a femoral–acetabular impingement, labral tear, hip osteoarthritis, hip avascular necrosis, iliopsoas bursitis, snapping hip, greater trochanter pain syndrome, core muscle injury, sports hernia, and osteitis pubis. An abdominal examination includes a Carnett test,94 an evaluation for potential hernias (including sports, inguinal, obturator, femoral, and umbilical hernias) or a persistent urachal remnant, an evaluation for trigger points in the rectus abdominus and external obliques, and an evaluation for allodynia or hyperalgesia along the ilioinguinal, iliohypogastric, and the genital branch of the genitofemoral nerves (Fig. 5). The presence of the anal wink reflex, a contraction of the external anal sphincter on stroking of the surrounding skin, is determined. This reflex is mediated by the pudendal nerve (S2-S4), which is often implicated in the pathogenesis of CPP. A cotton swab is used to perform the Q-tip test, identifying allodynia of the vulva. Allodynia in the top 1/3 of the vulva points toward involvement of the ilioinguinal or genitofemoral nerve, whereas allodynia in the lower 2/3 of the vulva points toward involvement of the pudendal nerve and the inferior cluneal branch and the perineal branch of coccygeus, piriformis, and puborectalis muscles can be assessed with a rectal examination.19,30 With the patient’s permission, an internal vaginal examination for women and a digital rectal examination42 for men is performed. In certain circumstances, such as high suspicion of deep infiltrative endometriosis or a chief complaint of coccydynia, a female patient may require a rectal examination. Full gynecological consultation with necessary workup and tests performed by a gynecologist is needed for female patients. Full urologic workup consisting of urinalysis, midstream culture, 2-glass prostate test, and prostate ultrasound performed by a urologist is needed for male patients.
5. Treatment
Besides aiding the diagnosis of CPP and determining its etiology, the physiatrist’s role in the multidisciplinary care team is to determine how each aspect of the condition impacts the patient and how each part can be treated or managed. This involves continuously trying to find the primary pain generator(s), while treating underlying central and peripheral sensitization and myofascial symptoms. It is important to treat both myofascial and neuropathic pain concomitantly, as they occur simultaneously. Moreover, true patient-centered health care may be achieved by shared decision-making.15 Owing to the dearth of extensive, quality research specifically addressing the management of CPP, effective treatment modalities for other neuropathic or chronic pain conditions are used. The biopsychosocial model incorporates the neuroscience processes of pain with psycho- social factors providing insights into approaching chronic pain heuristically.44 The ubiquitously recommended multimodal approach6,56,106 towards treatment of CPP includes pharmacotherapy, integrative options, minimally invasive procedures, and surgical treatment when appropriate.
5.1. Pharmacological management
The management of CPP requires a multimodal approach that focuses on symptom reduction. Treatment is often composed of both organ-specific treatment and central and peripheral neuromodulation. The categories of pharmacological agents reviewed include analgesics, topical agents, neuromodulators, and adjuvant therapies.
5.1.1. Analgesics
Short-term use of nonsteroidal anti-inflammatory drugs (NSAIDs) is first line in the management of acute pain “flares” in chronic pain conditions. Most research regarding CPP and NSAIDs demonstrates their efficacy for dysmenorrhea, specifically because of the effect of NSAIDs on the uterus during menses.18,71 Nonsteroidal anti- inflammatory drugs are nonselective inhibitors of the cyclo-oxygenase enzymes. They prevent the production of prostaglandins and thromboxane, providing peripheral pain relief. Selective cyclo- oxygenase-2 inhibitors have also been shown to reduce symptoms of primary and secondary dysmenorrhea, as well as CPP.34 Although acetaminophen is indicated for the treatment of myofascial pain, it does not seem to be helpful for chronic pain syndromes. Ennis et al.41 conducted a systematic literature review to evaluate the efficacy of acetaminophen when used for chronic pain conditions which showed little supporting evidence and recommended the assessment of continuous efficacy in many patients using acetaminophen worldwide.
5.1.2. Topical Agents (1) Topical analgesics may be effective for relieving pain in some patients with chronic musculoskeletal or neuropathic conditions such as osteoarthritis, postherpetic neuralgia, HIV-neuropathy, and diabetic neuropathy. Meta-analyses assessing the efficacy of diclofenac, ketoprofen, and capsaicin have reported positive results for these conditions.36,37 The mechanism of action of capsaicin is believed to involve the desensitization of unmyelinated C nerve fibers implicated in some pelvic pain conditions. In a clinical trial, the capsaicin application to the skin overlying the perineal body resulted in symptom reduction for 16 of the 22 men with chronic prostatitis or CPPS at the 7-day follow-up and the mean National Institutes of Health Chronic Prostatitis Symptom Index Score decreased from 27 to 16 (P , 0.01). A limitation of this study, however, is its small sample size suggesting the need for additional larger and more controlled studies.108 (2) The topical anesthetics, lidocaine and bupivacaine, act as sodium channel blockers. Their efficacy in treating vulvodynia, a common feature of CPP, has been demonstrated by Zolnoun et al.116 in a study of 61 women. After a mean of 7 weeks of nightly treatment, 76% of women reported ability to have intercourse, compared with 36% before treatment (P 5 0.002). A randomized, double-blind, clinical trial is warranted. (3) Selective peripheral voltage-gated sodium channel blockers are being developed for the treatment of neuropathic pain, not specifically CPP. The potential power of targeting specific voltage-gated sodium channels to reduce pain sensations is strongly supported by pharmacological studies in cells and animal models and by genetic channelopathy studies in rare inherited mutations linked to abnormal painful neuropathy.17,38
5.1.3. Neuromodulators For CPP that is unresponsive to targeted therapy or that is nonspecific, the field of pain medicine accepts the importance of the role played by pathologic central pain processing. Medications which alter circulating neurotransmitters believed to underlie that imbalance are widely used. These neuromodulators include tricyclic antidepressants, serotonin–norepinephrine reuptake inhibitors (SNRIs), gabapentinoids, and other antiepileptics.
(1) Tricyclic antidepressants are first-line agents for neuropathic pain.76 They act by inhibiting the reuptake of serotonin and norepinephrine, relieving neuropathic pain and depression, the most common mood disorder associated with chronic pain.9 Amitriptyline is one of the most used agents in treating neuropathic pain syndromes. 56 women with CPP were investigated with a 2-year follow-up at the Vienna Medical University Hospital where they all experienced significant pain relief during the observation period. After 6, 12, and 24 months, pain relief was significantly better in patients receiving gabapentin either alone or in combination with amitriptyline (amitriptyline: 0 months, 7.3 6 1.5; 6 months, 2.2 6 1.6; 12 months, 2.2 6 1.6; and 24 months, 3.4 6 0.9 and amitriptyline–gabapentin: 0 months, 7.6 6 0.8; 6 months, 1.3 6 0.9; 12 months, 1.7 6 1.0; and 24 months, 2.3 6 0.9).92 Tricyclic antidepressants however must be used with caution in patients with a history of cardiac or neurologic comorbidities because of its anticholinergic adverse effects.49 (2) The anticonvulsants gabapentin and pregabalin have demonstrated efficacy in treating other chronic pain syndromes and are approved for their treatment by the U.S. Food and Drug Administration.32,33 Gabapentinoids bind to the alpha- 2-delta subunit of voltage-gated calcium channels, de- creasing glutamate, norepinephrine, and substance P re- lease in the setting of neural hyperactivation.102 In a pilot study regarding the use of gabapentin for CPP, women in the treatment group reported greater pain reduction (Brief Pain Inventory difference 1.72 points, 95% CI: 0.07–3.36) and mood improvement at the 6-month follow-up than those in
the control group.66 This however was a feasibility study and not large enough to produce reliable estimates of treatment effects. Several studies regarding the mechanism of action of
gabapentinoids when used for chronic pain, allodynia, and hyperalgesia point towards the interruption of central sensitization.111 As CPP etiology likely involves central sensitization, the use of gabapentinoids as a treatment modality is intuitive. However, a double-blind, placebo- controlled trial of women with CPP randomly assigned (153 to gabapentin and 153 to placebo) showed no benefit with gabapentin and was associated with higher rates of side effects compared with the placebo. Thus, it is vital physicians consider alternatives to gabapentin given the evidence of possible harms and uprise of abuse reports.53
(3) Serotonin–norepinephrine reuptake inhibitors, such as duloxetine and venlafaxine, increase centrally available nor- epinephrine, which seems to have an analgesic effect. The Canadian Pain Society listed duloxetine and venlafaxine among the first-line agents recommended for treating neuropathic pain.76 A small, unblinded trial suggested improved symptom relief (significant improvement in the National Institutes of Health Chronic Prostatitis Symptom Index [NIH-CPSI] pain and quality of life subscores and NIH-
CPSI total score), decreased depression, and better quality of life (significant improvement in the Hamilton Anxiety Scale and the Hamilton Depression Scale scores [P , 0.01, respec-
tively]) for men with CPP when duloxetine was added to an existing drug regimen.46,113 (4) Antiepileptic sodium channel blocking agents, such as phenytoin, carbamazepine, and lamotrigine, reduce membrane excitability of all neurons and diminish spontaneous firing of sensory neurons.17 A pilot study found a statistically significant reduction in pain (McGill Pain Rating Index, P 5 0.003; McGill pain intensity [VAS, visual analogue scale], P ,
0.0001; and pelvic pain intensity, P , 0.0001) and improvement in mood (Hamilton Depression, P 5 0.002) and anxiety
symptoms (Hamilton Anxiety, P 5 0.02) among women taking lamotrigine, particularly for those with vulvodynia. Limitations of this pilot study included its open-label design with a lack of control group and a small sample size. Also, the results were based on a single cohort from a referral-based pelvic pain clinic which may have introduced a sample bias and limited the generalizability of the findings to a more diverse CPP population.73
5.1.4. Adjuvant pharmacotherapies (1) In a systematic review regarding the use of cannabinoids for medical purposes, moderate-quality evidence was found to support their use in treating chronic neuropathic pain; however, an increased risk of many adverse effects was also shown.109 No studies specifically addressing the treatment of
CPP with cannabinoids were found. (2) Diazepam suppositories are often used as an off-label therapy in the management of pelvic floor hypertonia. Studies regarding their efficacy for pelvic hypertonicity and/ or dysfunction are limited and show mixed results.26,51,64,86 A study of 49 randomized women (25 in the diazepam arm and 24 in the placebo arm) showed no difference in scores between the treatment groups after 4 weeks (50 vs 39 mm, for diazepam and placebo, respectively; P 5 0.36).51 Contrastingly, a study of 21 women taking diazepam for a month showed a decrease from 5.9 to 2.2 in the average pain score. The small sample size of this study limits any widespread conclusions.26 A key pharmacokinetic
evaluation showed lower serum plasma concentration and bioavailability of vaginally administered diazepam compared with oral use in 8 healthy volunteers. Its prolonged half-life consequently favors intermittent use, allowing participation in physical therapy and intimacy. A limitation of this investigation is the lack of a pure pharmacokinetic study.64 In addition, a retrospective chart review on 26 patients with high-tone pelvic floor dysfunction and sexual pain receiving diazepam suppositories in addition to pelvic physical therapy and intramuscular trigger point injections reported 25 patients with subjective improvement, and 6 of 7 sexually active patients returned to intercourse. Vaginal diazepam suppositories created clinically significant improvement (sexual pain assessed on FSFI and serial VAS-P improved with diazepam by 1.44 on a 10-point scale, P 5 0.14) compared with physiotherapy alone.86 This suggests diazepam suppositories may provide desirable results when combined with other therapies. 5.2. Integrative strategies Integrative management, including physical therapy, cognitive
behavioral therapy (CBT), physical activity, yoga, acupuncture, and peripheral neuromodulation, is used in conjunction with pharmacotherapy and minimally invasive procedures.
5.2.1. Physical Therapy For patients with CPP, the first-line treatment is pelvic floor physical therapy.88 Physical therapy, including those without targeted findings, promotes improved balance, movement, and neuromuscular function which all impact the patient’s quality of life. These improvements may also downregulate the pathologically altered pain processing systems. Pelvic floor physical therapy has been shown to reduce symptoms in up to 72% of patients, even among those without improvement from previous treatment modalities.7
5.2.2. Cognitive behavioral Therapy
As depression and anxiety are extremely common among patients with chronic pain, including those with CPP,46 it is important to address the patient’s mental health when establishing a treatment plan. There is evidence that depression and pain have a bidirectional negative impact. The presence of depression causes worsening of pain symptoms and vice versa. Thus, addressing the psychological aspect of pain conditions is important for the improvement of physical symptoms.9 The Society of Obstetricians and Gynecologists of Canada published guidelines for managing CPP. Among the key recommendations listed therein, the need for multidisciplinary or multimodal care that includes a psychological component such as CBT.56 Cognitive behavioral therapy is a broad term for therapies that involve a focus on changing behaviors and thoughts to change affective states. One study of 118 patients found “reduced overall pain severity and pain during intercourse, increased sexual satisfaction, enhanced sexual function, and less exaggerated responses to pain,” after a course of CBT.20 One limitation of CBT is its time-intensive nature. A 2019 study demonstrated significant gains in treatment outcomes addressing psycho- education and goal setting, pacing, and relaxation training of a short-term CBT intervention delivered in a primary care setting.14 Therefore, having a psychotherapist who is trained to deliver these services alongside physicians providing necessary medical
5.2.3. Physical activity
Traditionally, exercise is an integral part of the rehabilitation of patients suffering from chronic pain conditions.67 A study of 231 men diagnosed with CPP randomized into 2 groups of aerobic exercise and placebo of stretching demonstrated significantly superior improvement with aerobic exercise compared with the placebo group after 18 weeks. Thus, validating aerobic exercise as a viable treatment option which should be further investigated in a larger study with longer follow-up.47 Another study focusing on the prevention of CPP analyzed the relationship between physical activity and incidence of CPPS in a large cohort of male health professionals. An inverse association between total leisure-time physical activity and the risk of developing CPPS was observed suggesting that higher levels of leisure-time physical activity may lower risk of CPPS.114
5.2.4. Yoga
Incorporating yoga as a form of exercise seems to be helpful for various chronic pain conditions, including CPP and dysmenorrhea. When compared with controls, women who participated in a yoga program experienced a statistically significant reduction in pain and improvement in psychosocial quality of life.93,112
5.2.5. Acupuncture
Acupuncture is a form of sensory nerve stimulation associated with rapid and long-lasting effects in CPPS treatment.48,81 One study demonstrated that acupuncture was associated with reduced dysmenorrhea in women with endometriosis-related pelvic pain.115 A trial of 100 patients with CPPS randomized to receive acupuncture or “sham acupuncture” at points adjacent to the correct acupoints demonstrated a significant decrease in NIH-CPSI scores in both groups, but the improvement was significantly greater in the active acupuncture group (.50% decrease in NIH-CPSI score).90 Another randomized control trial of 44 participants proved the acupuncture group was 2.4-fold more likely to experience continuing benefits than participants who received sham acupuncture.65 Although its efficacy is undetermined, there is believed to be minimal risk involved for patients who are interested in a trial of acupuncture for CPP.
5.2.6. Peripheral neuromodulation
Peripheral neuromodulation involves the delivery of electrical
stimulation to a sensory nerve, which has been shown to suppress nerve fiber processing of nociception.40 Transcutaneous electrical nerve stimulation, percutaneous tibial nerve stimulation, sacral neuromodulation, and pudendal neuromodulation have all been used for various conditions. Currently, there is no evidence to support the use of these techniques for CPP conditions.
5.3. Nonsurgical interventional pain procedures
Research regarding interventional techniques for treating CPP is still in its infancy. Most of the evidence validating its efficacy is based on case reports and case series. There are also few comparison studies with other forms of treatment for CPP which would have better support for efficacy. Although the evidence is not robust, some studies do show promise. Nonoperative approaches for patients who experience limited response to physical therapy, medications, and CBT include trigger point injections, therapeutic nerve blocks, radiofrequency ablation (RFA), ethanol or phenol neurolysis, and botulinum toxin. (1) Trigger point injections most likely work by breaking up the taut bands of muscle, resetting shortened or contracted weak muscles and increasing blood flow. The theory of greatest acceptance involves the interruption of the hyperactive reflex arc by mechanical disruption of abnormal contractile elements in skeletal muscle fibers.5,63 Another possible mechanism is that the injectate causes muscle fiber release of intracellular potassium, resulting in aberrant nerve signal blockade. A prospective study out of the Cleveland Clinic included 18 women with CPP and levator ani trigger points who underwent transvaginal trigger point injections using a mixture of bupivacaine, lidocaine, and triamcinolone. This was followed by instructions for pelvic floor exercises to perform at home. Of the 18 participants, 13 demonstrated more than a 50% reduction in pain by the 3 month follow-up. Six of the total women included in this study were completely pain free at that time.63 A limitation of this study is its small sample size. A retrospective chart review of 101 women with CPP who received pelvic floor muscle trigger point injections showed a significant improvement in 77% of patients.13 A study of 37
men with CPP found that trigger point injections of lidocaine and bupivacaine buffered with sodium bicarbonate relieved symptoms in more than half of the patients and recommends their use as an adjunct to physical therapy. This study is limited by the small number of patients and the short follow-up suggesting the need for further studies to evaluate the long- term durability of this treatment.101 Our retrospective study of 73 women with CPPS who were treated with external ultrasound-guided trigger point injections to each muscle in the levator ani with peripheral nerve blocks using dexamethasone and lidocaine once a week for 6 weeks in conjunction with physical therapy showed statistically significant improvement in pain, specifically with intercourse and working.
Conceptually, our treatment protocol is based on the notion of neuroplasticity and the nervous system’s ability to change.78 Therefore, the goal of our protocol is to retrain the central and peripheral nervous system91 by decreasing neurogenic inflammation, decreasing muscle tension, and removing fascial restrictions by our 3-prone strategy. Some limitations of our study include a short follow-up time and a lack of a control group. In addition, our novel treatment strategy includes multiple concomitant treatments which have limited prior evidence, and further randomized controlled prospective studies are recommended77. (2) Serial therapeutic nerve blocks with local anesthetic and corticosteroid have shown success in many patients.27,100 The mechanism of action for this is multifactorial. One implicated mechanism involves the downregulation of sodium channel responsiveness on the primary afferent nerves after repeated exposure to the anesthetic. Other mechanisms include disruption of tight perineural connective tissue bands that correlate with the restricted mechanoreceptors described above and depletion of proinflammatory neuropeptides, such as substance P and histamine.97,98 Through these actions, serial therapeutic nerve blocks downregulate overexcited pathways that cause neurogenic pain. Terminating the aberrant pain feedback loop caused by hyperexcitable peripheral neurons allows peripheral nociceptors to return to their normal resting state. Nerve blocks are commonly used to target CPP pain generators, such as pudendal nerve, ilioinguinal nerve, genitofemoral nerve, superior hypogastric plexus, and ganglion impar, for diagnostic purposes. Nerve blocks are performed with guidance from palpable landmarks, computed tomography, ultrasound, or magnetic resonance neurography.1,43,50,70
Patients with pelvic pain and distribution of the peripheral nerve may benefit from nerve blocks for diagnostic or therapeutic reasons.55 Nerve blocks aid in the identification of pain generators by interventionalists, allowing them to proceed with a more definitive treatment such as neurolysis. However, there is evidence that nerve blocks themselves can yield a prolonged, significant pain reduction. In 1 prospective study, 20 patients underwent between 1 and 3 ilioinguinal or genitofemoral nerve blocks with a mixture of prilocaine and prednol-L. At the 12- month follow-up, 8 patients reported a VAS score of 0 and 6 patients reported a VAS score of 2, whereas the last 6 were nonresponders. Although favorable early postoperative pain control was provided, longer follow-up and more patients are needed to evaluate pain recurrence.1 Pudendal nerve blocks performed with ultrasound guidance allows for the identification of the pudendal nerve between the sacrospinous and sacrotuberous ligaments adjacent to the ischial spine, without radiation exposure.52,60 Fluoroscopic guidance can be used to reduce the risk of inadvertent intravascular injection.82 Kastler et al. demonstrated that pudendal nerve blocks can result in long-term pain relief. 95 patients had pudendal nerve infiltration at dual sites under CT guidance. One month after this procedure, 63.2% of patients achieved clinical success of greater than 50% improvement in pain. Clinical success remained in 50.5% of participants after 3 months and 25.2% after 6 months. Limitations include the retrospective nature and the lack of the control group. Furthermore, pain evaluation was made using simple scoring methods (VAS and SRI scores) which are subjective.59 (3) Neurolysis of the ilioguinal or iliohypogastric nerves, ganglion impar, and the superior hypogastric plexus, including RFA, pulsed radiofrequency ablation (PRFA), and phenol/ethanol infiltration, has very limited evidence among small sample sizes. (a) In several studies of individual research participants, RFA and cryoablation provided long-term pain relief without causing risk of neuroma formation.24,74 A 47-year-old man with 4/10 VAS remains pain free at his 2-month follow-up after receiving ultrasound-guided cryoablation.24 Similarly, a 58-year-old man with chronic ilioinguinal neuropathy was treated with PRFA and had lasting pain relief at his 3-month follow-up.74 Kastler et al. compared RFA vs local anesthetic infiltration of the ilioinguinal and iliohypogastric nerves for treating inguinal neuralgia in 42 patients.
Read the rest of the research and sources here.
