Brocha Brooks1,2,3,* | Kim Leishear1,2 | Rebecca Aronson1,2 | Melanie Howell1,2 |
Allen Khakshooy3 | Michael Pico4 | Allyson Shrikhande1,2
1 Pelvic Rehabilitation Medicine Clinical Research Foundation, New York, NY, USA
2 The Feinstein Institutes for Medical Research, Northwell Health, Manhasset, NY, USA
3 The Ruth and Bruce Rappaport Faculty of Medicine, Technion – Israel Institute of Technology, Haifa, Israel
4 Rusk Rehabilitation, NYU Langone Medical Center, New York, NY, USA
*Correspondence
Brocha Brooks, 18 East 41st St, Suite 2002, New York, NY, 10017, USA.
Email: [email protected]
KEYWORDS: A2M protein; Central sensitization; Chronic pain; Neurogenic inflammation; Neuropathic pain; Pelvic floor disorders;
Pelvic pain
Chronic pelvic pain syndrome (CPPS), defined as continuous or recurrent pain in the pelvic region lasting at least six months, which cannot be wholly attributed to a single organ or distinct pathology, 1 has a multifactorial etiology involving the gynecologic, urologic, gastrointestinal, musculoskeletal and/or neurologic systems. Aberrant pain signal processing and local tissue responses are contributive factors. 2 Current recommendations for management are multimodal and include physical therapy, pharmacotherapy, cognitive behavioral therapy, and interventional procedures.1
Alpha‐2‐macroglobulin (A2M), a plasma glycopotein with protease inhibition, antioxidant, and anti‐inflammatory properties,3 has shown potential for reducing pain and inducing healing in several musculoskeletal and peripheral neural conditions.4,5 As CPPS involves neurogenic inflammation which leads to peripheral and central sensitization,1 this study was performed to determine the efficacy of adding A2M to an existing CPPS treatment protocol for further
symptom relief.
With IRB approval from the Feinstein Institutes for Medical Research (IRB No. 17–0761), 19 patients that were under care for
CPPS at a physiatry practice between December 2017 and January 2018 were retrospectively reviewed. Inclusion criteria were prior treatment with a series of outpatient ultrasound‐guided trigger point injections to the levator ani sling and peripheral nerve blocks.6 Patients were excluded due to pregnancy, malignancy, or if less than a 30% improvement was observed after completing the prior treatment protocol aimed at decreasing neurogenic inflammation.6 Because A2M targets neuropathic and inflammatory mechanisms, excluding those with little improvement from previous treatments targeting these pathways was deemed important.
After informed consent was obtained from the patient, blood was drawn from the antecubital fossa for centrifugation and filtration via an Autologous Platelet Integrated Concentration (APIC) system (Drucker Diagnostics, Philipsburg, PA, USA) designed to separate components and concentrate A2M contained in plasma. Under aseptic technique, and with the patient in the prone position, approximately 5 mL of 1% lidocaine, followed by approximately 5 mL of autologous A2M, was placed into Alcock’s canal using ultrasound guidance. A hydro-dissection technique was used (Fig. 1), allowing the injectate to separate the pudendal nerve from the surrounding tissue, thus disrupting the adhesions responsible for hypersensitivity.7 The present study focused on the pudendal nerve as the primary instigator in CPPS,8 though the technique can be applied to other pelvic nerves for maximal benefit. This procedure was performed bilaterally for all except two participants who suffered with distinctly unilateral pain.
Pain and function were assessed via the Visual Analogue Scale (VAS) and Functional Pelvic Pain Scale (FPPS) before treatment and at a follow‐up visit after the injection. The FPPS assesses function relating to bladder, bowel, intercourse, walking, sleeping, working, running, and lifting. Scores for all categories were summed to obtain a total function score. Categories missing a score for a given participant were excluded from that participant’s total function score. The Wilcoxon signed‐rank test was employed to determine significance (α=0.05) of pain and total function changes by SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
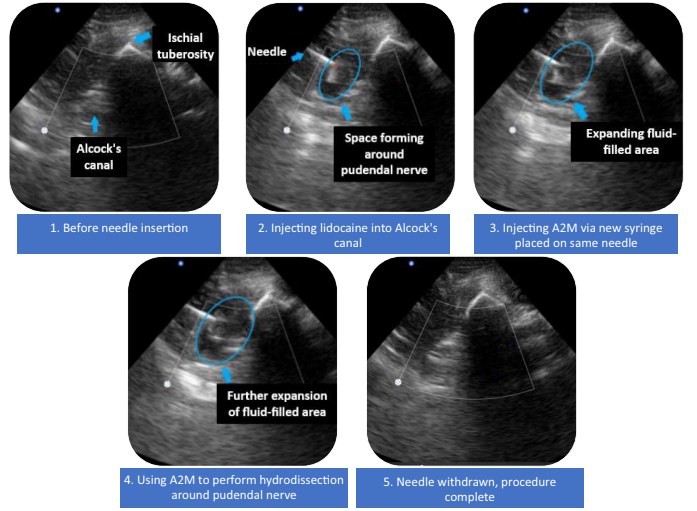
FIGURE 1 Ultrasound images of A2M placement to Alcock’s canal with hydrodissection technique. Abbreviations: A2M, alpha‐2‐
macroglobulin
Eight male and eleven female patients (Table S1) underwent ultra-sound‐guided perineural A2M injections with hydrodissection into Alcock’s canal. Patients returned to work the same day of the procedure. No adverse events were noted. Follow‐up data were measured up until the 20th postoperative week, with a mean of 9.4 weeks (SD 3.2). The mean age of participants was 38.6 years (SD 10.0) and the mean duration of pain was 5.1 years (SD 4.4). Pain relief was reported by 10 patients (52.6%) and improved total function by 12 patients (63.2%). The change in total FPPS scores was statistically significant (P=0.015), though that of VAS scores was not (P=0.353). Score changes for all categories are displayed in Figure 2.
The present study showed a statistically significant improvement in total pelvic function. This is likely the effect of A2M, a protease inhibitor, reducing neurogenic inflammation around the pudendal nerve which occurs in cases of CPPS.8 In addition, promoting a better environment for healing of the pudendal nerve will ultimately terminate the peripheral and central sensitization processes that occur in CPPS.1 Of note, patients with chronic pelvic pain and pudendal neuralgia rarely awaken at night due to pelvic pain symptoms, therefordecreasing neurogenic inflammation around the pudendal nerve will not change sleep patterns.9 This was observed in the current study by the large number of patients who experienced no sleep disturbance before or after treatment (Fig. 2).
Our study demonstrated the potential use of perineural A2M injections as an adjunctive treatment for reducing pain and improving pelvic function in patients with CPPS. It has laid the foundation for future research involving a larger sample size and longer follow‐up.
AUTHOR CONTRIBUTIONS
BB was responsible for data collection, data analysis, and writing of the manuscript. KL, RA, and MH contributed to the conduction of study and data collection. AK was responsible for data analysis and writing of the manuscript. MP contributed to the writing of the manuscript. AS was responsible for the study design, planning, data collection and writing of the manuscript. All authors approved of the final version of the manuscript.
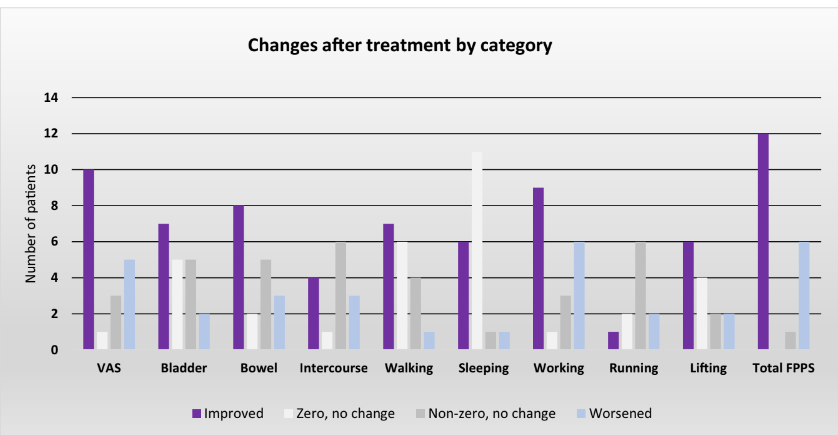
FIGURE 2 Number of participants who demonstrated an improvement, a decline, or no change after treatment for each category of pain and function. Zero, no change: Patients who reported no pain or dysfunction before treatment and no new onset of deficits in that category after treatment. Non‐zero, no change: Patients who reported pain or dysfunction before treatment with no change in severity after treatment. Abbreviations: VAS, Visual Analogue Scale; FPPS, Functional Pelvic Pain Scale
CONFLICTS OF INTEREST
The authors have no conflicts of interest.
REFERENCES
1. Engeler D, Baranowski AP, Berghmans B. EAU guidelines: Chronic pelvic pain. Uroweb. Published 2003. Updated 2020. https://uroweb.org/guideline/chronic‐pelvic‐pain. Accessed May 5, 2020.
2. Carey ET, As‐Sanie S. New developments in the pharmacotherapy of
neuropathic chronic pelvic pain. Future Sci OA. 2016;2:FSO148.
3. Rehman AA, Ahsan H, Khan FH. Alpha‐2‐macroglobulin: A physiolog-
ical guardian. J Cell Physiol. 2013;228:1665–1675.
4. Cuellar JM, Cuellar VG, Scuderi GJ. Alpha‐2‐macroglobulin:
Autologous protease inhibition technology. Phys Med Rehabil Clin N Am. 2016;27:909–918.
5. Jordan S, Lovine J, Kuhn T, Gelabert H. Neurogenic thoracic outlet syndrome and other forms of cervical brachial syndrome treated with plasma concentrate enriched for alpha 2 macroglobulin. Pain Physician. 2020;23:229–233. 6. Plavnik K, Tenaglia A, Hill C, Ahmed T, Shrikhande A. A novel, non‐opioid treatment for chronic pelvic pain in women with previously treated endometriosis utilizing pelvic floor musculature trigger point injections and peripheral nerve hydrodissection. PM&R.
2020;12:655–662.
7. Cass SP. Ultrasound‐guided nerve hydrodissection: What is it? A
review of the literature. Curr Sports Med Rep. 2016;15:20–22.
8. Prendergast SA, Weiss JM. Screening for musculoskeletal causes of
pelvic pain. Clin Obstet Gynecol. 2003;46:773–782.
9. Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J.
Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn. 2008;27:306–310.
SUPPORTING INFORMATION
Additional supporting information may be found online in the Supporting Information section at the end of the article. Table S1. Patient demographics and individual response to treatment.
